Breast Reconstruction
“I have breast cancer… and then what?” This is the title of the book by Professor Pascal Bonnier and photographer Florian Launette, published in 2007. Testimonies, photographs, women’s faces; for the first time, the general public was shown breasts operated on for cancer and then reconstructed. The goal was to demystify and reassure, and it worked.
All these women who testify and show their torsos have gone through every step, so why not me, one thinks. When it “hits us”, we have an intense need for information. That is why this section explains not only the surgical techniques but also provides links to various associations; my secretary can also put you in contact with people who have been through the same experience.

The different types of breast reconstruction
After a mastectomy several surgical options can restore the breast. The choice of technique depends on the patient’s wishes her anatomy and the oncological treatment received.



Ready to book an appointment?
General information
There are two types of breast reconstruction:immediate breast reconstruction (IBR) and delayed breast reconstruction (DBR).
IBR is performed during the same surgical procedure as the mastectomy. It is the most modern approach and can be offered to patients more and more frequently. Immediate breast reconstruction can be carried out using a flap, a breast implant, a tissue expander, or a simple transfer of autologous fat.
Sometimes the mastectomy preserves the areola and the nipple, which avoids the need to reconstruct the nipple areola complex. This is the case for preventive surgery in women carrying a genetic mutation (BRCA1, BRCA2), such as Angelina Jolie, or in cases of small cancers located far from the nipple.
Delayed breast reconstruction is performed approximately one year after breast removal, depending on the additional treatments required to cure the cancer (radiotherapy, chemotherapy). The techniques used are similar to those of immediate reconstruction and, in these cases as well, autologous fat transfer has helped improve aesthetic results. Because a breast is not reconstructed to look unattractive. Aesthetic criteria are always present in reconstructive surgery.
Make an appointement
If you wish to benefit from a personalised consultation with Dr Marianne Prevot.

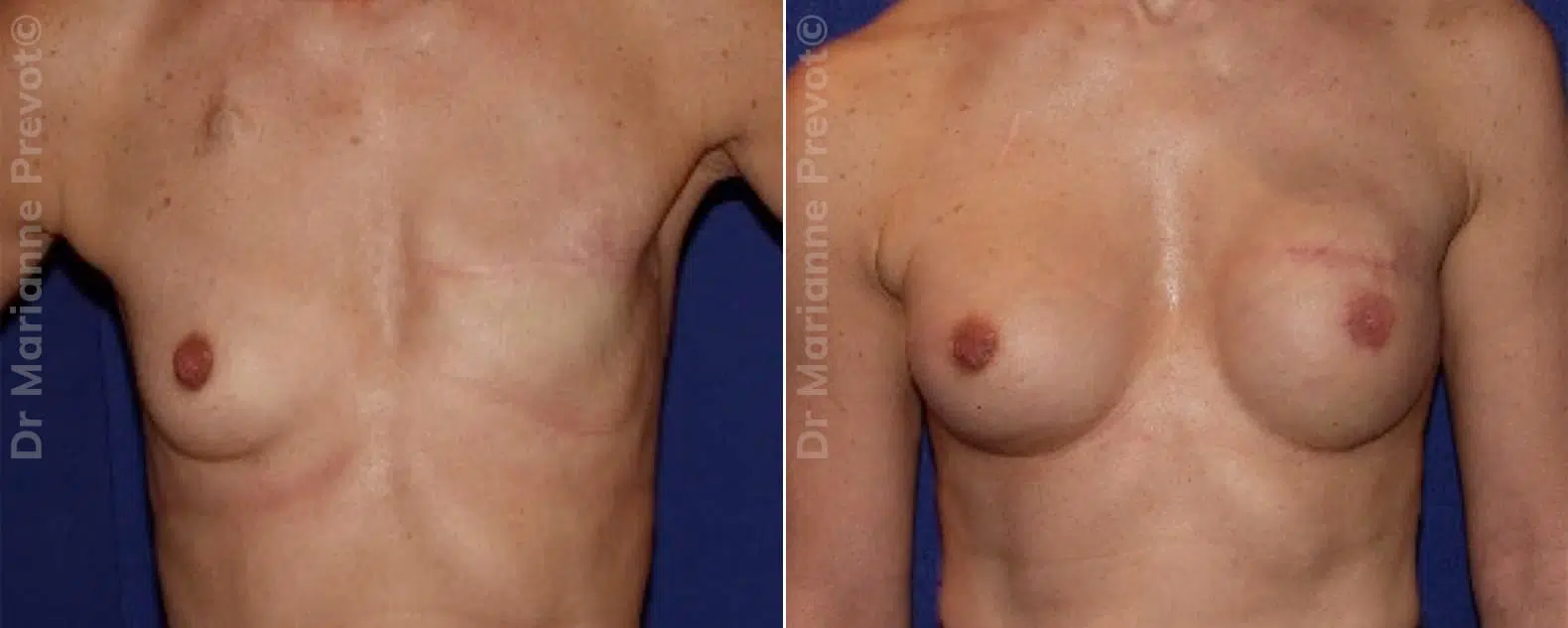
Results


Types of breast reconstruction
Here are the main techniques used today, adapted to each situation and to each patient.
Breast reconstruction with implants
Reconstruction with breast implants is one of the most commonly used techniques. It consists of placing a silicone implant or a tissue expander to restore breast volume and shape. This procedure is often performed as immediate reconstruction, meaning at the same time as the mastectomy. Simple and effective, it offers natural looking results and a relatively short recovery time. It can be combined with autologous fat transfer to refine the aesthetic outcome.
Breast reconstruction using a latissimus dorsi flap and fat transfer
This technique uses a latissimus dorsi muscle flap taken from the back to reconstruct the breast. When combined with fat transfer, it allows the creation of a breast that is natural in both shape and texture. Ideal for patients who do not wish to use implants, this method also has the advantage of reinforcing the chest wall. However, it requires a more complex procedure and a longer recovery period.
Breast reconstruction with free flap and microsurgery
Free flap reconstruction is an advanced technique that uses tissue taken from another part of the body, such as the abdomen (DIEP flap). Thanks to microsurgery, blood vessels are reconnected to ensure tissue viability. This method allows the creation of a very natural breast, with a tactile sensation close to that of a non operated breast. Nevertheless, it requires specific surgical expertise and a longer hospital stay.
Fat injection or autologous fat transfer :“fat transfer”
Autologous fat transfer, also known as fat transfer, involves harvesting fat from another area of the body (such as the thighs or abdomen) and reinjecting it into the breast. This technique is often used as a complement to another reconstruction method, to refine the result or correct asymmetries. Minimally invasive, it provides a natural and harmonious appearance.
Reconstruction of the areola and nipple
Reconstruction of the areola and nipple is often the final stage of the process. It can be performed using skin grafts, medical tattooing, or microsurgery. Although subtle, this step plays a key role in restoring body image and self confidence.
Each technique has its advantages and specific features. Together, we will choose the one that best suits your needs and your personal journey. Do not hesitate to contact me to discuss your options or to book an appointment with my secretary.
DR marianne prevot
Dr Marianne prevot is a plastic surgeon in Geneva specializing in aesthetic reconstructive pediatric and dermatologic surgery. With more than 20 years of experience she combines medical expertise scientific commitment and a human centered approach.
Her practice is based on harmony between body and mind with an ethical and balanced vision of surgery.




